April 28, 2026
By Yossi Bar, CEO and Founder of LEM Surgical; April 28th, 2026.
The field of surgical robotics is currently navigating a fundamental crossroad. For three decades, the industry has been defined by soft tissue platforms that rely on remote manipulation and human in the loop control. However, as global healthcare systems confront the dual crises of an aging population and a shrinking surgical workforce, the transition toward full autonomy has moved from a technological luxury to an absolute necessity. This article argues that hard tissue robotics is uniquely positioned to lead this coming paradigm shift through the realization of Physical AI.
While soft tissue continues to present challenges due to its stochastic and unpredictable deformation, hard tissue provides a stable, rigid environment that allows for precise, autonomous robotic planning and execution.
By integrating the technological pillars of bimanual humanoid architecture, advanced proprioception, and instrument agnosticism, hard tissue systems are poised to leapfrog soft tissue robotics to achieve the first true realization of autonomous surgery.
The article is organized into the following chapters:
- Background examines the demographic surge and surgical workforce shortage that make autonomous robotics an absolute essence for modern healthcare.
- The Historical Divergence analyzes the thirty-year evolution of soft tissue teleoperation versus the development of hard tissue autonomous logic.
- The Physics of Predictability details the fundamental biomechanical differences between the stable nature of hard tissue and the unpredictable behavior of soft tissue, identifying bone as the ideal substrate for Physical AI.
- The Challenge of Soft Tissue Autonomy explains why the complexity of sensing and tracking deformable organs in real time creates a significant bottleneck for autonomy.
- The Strategic Leapfrog describes how new form factors, such as the LEM Surgical bimanual humanoid architecture, serve as the physical embodiment of Surgical Physical AI, to bypass the limitations of previous robotic generations.
- Background: The Demographic and Professional Imperative
The modern surgical landscape is facing a systemic challenge that cannot be resolved through incremental improvements in manual dexterity alone. Autonomous surgical robotics is not merely a complementary addition to modern medicine; it is an absolute essence required to maintain the viability of healthcare delivery.
The Demographic Surge
We are currently witnessing a global demographic shift. Data from the World Health Organization [6] indicate that the population aged 60 and over is expected to reach 2.1 billion by 2050. This demographic shift is accompanied by a massive increase in the demand for surgical interventions, specifically in specialties related to age induced degeneration, such as orthopedic joint replacements and complex spinal procedures. The volume of these cases is expanding at a rate that far exceeds the capacity of traditional surgical models. As established in previous foundational analyses, the sheer scale of the elderly population requires a shift from human dependent surgery to system dependent outcomes.
The Aging Surgical Workforce
Simultaneously, the global surgical workforce is facing its own aging crisis. According to reports from the Association of American Medical Colleges [1], the industry faces a projected shortage of up to 86,000 physicians by 2036. A significant percentage of active surgeons are themselves approaching retirement age. This creates a situation where fewer practitioners are tasked with treating a larger, more complex patient population. In this environment, the traditional one-to-one model of surgery is no longer sustainable. Autonomy offers the only viable path to scale surgical expertise, reduce human variability, and manage the high volumes required by an aging society [1].
- The Historical Divergence: 30 Years of Evolutionary Paths
To understand why hard tissue robotics is taking the lead in autonomy, we must examine the divergent evolutionary paths taken by the industry over the last thirty years.
Soft Tissue: The Bypassed Logic of Teleoperation
Beginning three decades ago, soft tissue robotics evolved primarily as a solution for remote manipulation. Systems such as the da Vinci platform were designed to overcome the limitations of traditional laparoscopy by providing 3D visualization and wristed dexterity. However, these systems essentially bypassed the most difficult problem in robotics, which is the autonomous closed loop control.
By keeping the surgeon at a console, the robot functioned as a sophisticated extension of the human hand. The operating surgeons themselves closed the robotic loop with their eyes, using their own neural processing to interpret visual feedback and adjust their movements in real time.
At that time, the development of autonomous machine logic was deemed unnecessary for clinical success. The original design was specifically engineered to mimic the human operational mode, incorporating two operating hands and a 3D vision system similar to human perception. Consequently, the basic teleoperated design leapfrogged the initial architecture of hard tissue robots, which were limited to single arm configurations and the much more difficult task of closing the loop autonomously. While hard tissue robotics was forced to evolve through the complexities of machine intelligence, soft tissue systems relied on the human operator to fill the gap where logic was missing.
Hard Tissue: The Struggle for Autonomous Execution
In contrast, hard tissue robotics attempted the significantly harder task from its inception. Early prototypes, such as the ROBODOC system, were designed for active, autonomous tasks like milling the femur for hip replacements [5]. These systems required automatic robotic loop closing, which meant they had to register preoperative imaging to the patient’s physical anatomy and execute a plan without continuous manual guidance.
Because this was a much more difficult robotic task from a software and safety perspective, hard tissue robotics evolved more slowly. It remained largely confined to single arm systems with very little functionality and strict safety constraints. While soft tissue robotics was perfecting the interface, hard tissue robotics was perfecting the logic. This long period of evolution was necessary to master the complexities of rigid body mechanics and registration, setting the stage for the current leapfrog effect.
- The Physics of Predictability: Hard versus Soft Tissue
The fundamental barrier to autonomy in surgery is the biomechanical behavior of the tissue itself. The difference between bone and organ tissue dictates the speed at which a robot can assume control.
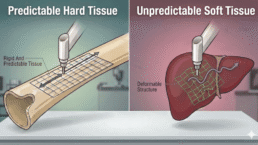
The Basic and Fundamental Difference
There is a profound difference between how hard tissue and soft tissue react to surgical intervention. Hard tissue is a predictable medium that behaves as a rigid body. Once a robot has accurately registered the patient’s anatomy, the geometric relationship between the tool and the tissue remains constant. Hard tissue does not deform when touched, providing a stable environment where preoperative plans can be translated directly into intra operative execution [7].
This stability allows Physical AI to move from theoretical modeling to reliable practice. Unlike digital AI, which processes information in a virtual space, Physical AI must understand and interact with the physical laws of its environment.
Soft tissue, conversely, is inherently unpredictable. When a surgical instrument, or even a retracting finger, touches a soft organ, that organ moves in a random manner. This movement is not uniform, as it involves deformation, sliding, and shifting. This fundamental predictability allows hard tissue robots to close the control loop autonomously with much higher precision than is currently possible in a soft tissue environment.
- The Challenge of Soft Tissue Autonomy
Because of the physics described above, soft tissue robotics will require significantly more time to transition from remote manipulation to full autonomy.
The Sensing and Perception Bottleneck
The bottleneck for autonomy in soft tissue is not only in the required computational power but also in the immense sensing capabilities, including vision and force. The challenge is that in surgery, no procedural deviations or outliers are acceptable. For a robot to be autonomous in this environment, it must possess real time perception and execution capabilities, which are at the minimum, as fast and accurate as of a human operator.
Recent peer reviewed research into uncertainty quantification for soft tissue manipulation has highlighted that system failures often stem from the partially observable and deformable nature of the environment [8]. It is extremely difficult for robots to predict and react to tissue motion in real time [2]. The challenge is not only to predict the motion but also to track and follow it in real time. The system must predict how a lung will deflate or how a liver will slide when pushed. Currently, the computational power and sensor fusion required to model these stochastic movements in real time remain major obstacles. This is why soft tissue systems, which are today based on remote manipulation, will continue to rely on human operators to bridge the gap in real time perception for the foreseeable future.
- The Strategic Leapfrog: The Evolution of Form Factor
While hard tissue is fundamentally closer to automation, a new form factor is required to unlock this potential. The emergence of new form factor robots, as exemplified by LEM Surgical technology [4], represents the catalyst for the coming leapfrog.
Humanoid Bi-manual Architecture
As discussed in previous articles regarding architectural shifts, the transition to a humanoid bi-manual architecture is critical [3,4]. Traditional hard tissue single arm robotic systems serve primarily as instrument guides and holders. In contrast, a bi-manual humanoid architecture allows for more comprehensive robotic work by integrating dual arm coordination. For example, one arm can hold and stabilize the hard tissue while the second performs accurate and controlled bone milling, drilling or sawing on the now stabilized bone structure. Furthermore, clinical demonstrations of humanoid robots as surgical assistants have established that the anthropomorphic form factor is feasible for navigating confined surgical workspaces and maintaining stable instrument positioning [9].
The Role of Proprioception: The Intelligence of Physical AI
Advanced proprioception is the second pillar of this technological shift [3]. For a robot to operate autonomously in a hard tissue environment, it must possess an internal sense of its own position and the forces being applied. This goes beyond simple visual tracking, which can be obscured in a surgical site. Proprioception in this context represents the embodiment of Physical AI, encompassing both kinematical awareness and sensorial feedback [3].
High fidelity proprioceptive sensors enable the robot to perform internal state estimation, effectively feeling the interface between the tool and the bone while maintaining a precise, real-time map of its own posture and spatial configuration. This holistic understanding of the physical state allows the autonomous loop closing to be grounded in physical reality rather than relying solely on optical data. By sensing resistance and micro vibrations during bone preparation, the robot can adjust its torque and speed in real time, minimizing the risk of unintended outcomes that are unacceptable in a clinical setting.
Instrument Agnosticism
Finally, the leap toward autonomy is supported by instrument agnosticism [3]. Previous generations of hard tissue robots were often closed systems, limited by proprietary tools. Modern autonomous platforms are designed to be agnostic, allowing them to utilize a wide range of validated surgical instruments. This flexibility ensures that the robot can be integrated into existing workflows without forcing a total overhaul of surgical hardware, making the transition to autonomy more feasible for healthcare institutions.
Bottom Line
Hard tissue is inherently closer to automation because it lacks the uncertainty of tissue deformation. However, the bottleneck until now has been the form factor. The emergence of new form factor robots, characterized by bimanual humanoid architecture, proprioception, and instrument agnosticism, will enable hard tissue robotics to leapfrog above soft tissue teleoperation.
Conclusion: The Dawn of Autonomous Surgery
The coming paradigm shift in surgery will not be led by the systems that currently dominate the market. While teleoperated soft tissue robots have provided significant benefits, they are fundamentally limited by the unpredictable nature of the tissue they treat. They remain tethered to the human brain to manage the outliers that occur when soft organs move.
Hard tissue robotics is the true pioneer of the autonomous era. By focusing on predictable, rigid structures and utilizing the emerging power of bimanual humanoid systems, these robots will be the first to achieve the levels of Surgical Physical AI required to address the global surgical crisis.
This leapfrog effect will redefine the surgical workflow, moving the surgeon from a direct manual operator to a high-level supervisor of autonomous systems.
Hard tissue robotics is no longer just a tool for orthopedics; it has become the essential foundation for the future of Physical AI across all medical interventions.
This article was written by a Physical Human with the assistance of Artificial Intelligence.
References
- AAMC. (2024). The Complexities of Physician Supply and Demand: Projections from 2021 to 2036. Association of American Medical Colleges. https://www.aamc.org/media/75231/download
- Haidegger, T. (2019). Autonomy for Surgical Robots: Concepts and Paradigms. IEEE Transactions on Medical Robotics and Bionics, 1(2), 65-76. https://doi.org/10.1109/TMRB.2019.2913282
- LEM Surgical. (2025). Proprioception and Instrument Agnosticism in Autonomous Systems. (Company Whitepaper). https://lemsurgical.com/next-generation-surgical-humanoids-from-trajectory-guide-to-therapeutic-executor/
- LEM Surgical. (2026). The Paradigm Shift in Hard Tissue Robotics: Bimanual Humanoid Architecture and Autonomous Closed-Loop Control. (Company Whitepaper). https://lemsurgical.com/the-democratization-of-care-scaling-the-artisan-surgeon-through-physical-ai/
- Taylor, R. H., and Kazanzides, P. (2016). Medical Robotics and Computer-Integrated Surgery. Springer Handbook of Robotics, 1199-1222. https://www.researchgate.net/publication/227052875_Medical_Robotics_and_Computer-Integrated_Surgery
- World Health Organization. (2015). World report on ageing and health. ISBN 9789241565042. https://www.who.int/publications/i/item/9789241565042
- Zhu, Y., et al. (2026). ArthroCut: Autonomous Policy Learning for Robotic Bone Resection in Knee Arthroplasty. arXiv preprint. https://arxiv.org/abs/2603.03957
- Thompson, J., Richter, F., et al. (2025). Early Failure Detection in Autonomous Surgical Soft-Tissue Manipulation via Uncertainty Quantification. arXiv preprint. https://arxiv.org/abs/2501.10561
- Cho, S. M., Atar, et al. (2026). Humanoid Robots as First Assistants in Endoscopic Surgery. arXiv preprint. https://arxiv.org/abs/2602.24156